Alternatives to Hysterectomy Specialist
When medical therapy fails or is not an option for a variety of conditions, hysterectomy may be recommended. However, if you don’t feel ready for a hysterectomy procedure, you should know all of the alternatives available before making your choice.
Many general OB/GYN practices will recommend a hysterectomy immediately. At the Advanced Women’s Health Institute, we strive to make you aware of all reasonable options so that you can make an informed, comfortable decision about your body.
Ready to discuss your options? Schedule an appointment with us today.
FAQs on Hysterectomies
What is a hysterectomy?
Although there are multiple ways to perform a hysterectomy, the procedure always involves the surgical removal of your uterus. Depending on the reason for the hysterectomy, you may also have other parts of your reproductive system removed, including the cervix, fallopian tubes or ovaries.
What types of hysterectomy are there?
If you are opting for a hysterectomy, there are several options for your procedure, including:
- Abdominal hysterectomy: The abdominal hysterectomy is the most common approach to hysterectomy in the United States. About 50% of hysterectomies are abdominal. Hospital stay is 2-4 days, and patients typically take 6 weeks off work. Full recovery may take up to a year.
Centers that specialize in laparoscopic surgery have reported that more than 95% of hysterectomies for benign disease could be done laparoscopically instead of open.

- Vaginal hysterectomy: Vaginal hysterectomy is an alternative to abdominal hysterectomy when a woman has a normal-sized or only slightly enlarged uterus. Because no abdominal incisions are made, the patients tend to leave the hospital in 1-2 days. Women typically take 4 weeks off work.
- Laparoscopic-assisted vaginal hysterectomy: This procedure was introduced in the late 1980s so a woman with a larger uterus could avoid an open hysterectomy. The uterine vascular supply can be secured laparoscopically, thus avoiding the large abdominal incision. The uterus is then removed vaginally along with the cervix. The recovery is more rapid than abdominal hysterectomy and similar to vaginal hysterectomy.
- Total laparoscopic hysterectomy: This procedure was developed to allow the woman with an enlarged uterus to avoid an open hysterectomy. The uterine vascular supply can be secured laparoscopically, thus avoiding the large abdominal incision. The vagina is entered from above instead of from below. The uterus is then removed vaginally along with the cervix. The recovery is more rapid than abdominal hysterctomy and similar to vaginal hysterectomy.
- Laparoscopic supracervical hysterectomy (LSH): LSH is the least painful form of hysterectomy, with the fastest recovery, ever described. Women who have LSH can go home the day of the surgery up to 90% of the time. Office workers are back to work in as few as 4 days, typically working 4-6 hours. Most take 1-2 weeks off. Full recovery and return to exercise takes about 3-5 weeks. Women in physical jobs that require heavy lifting(more than 50 pounds) mostly need 6 weeks. Since the cervix is left the vaginal and pelvic floor anatomy is not altered. A study about pelvic prolapse repair reported fewer complications when the LSH was performed compared to Total laparoscopic hysterectomy.
- Laparoscopic intrafascial hysterectomy (LIH): LIH is similar to LSH for post op recovery. The difference is how the cervical canal is treated. Critics of LSH focus on continued risk of cervical cancer and post operative cervical bleeding, either cyclic or random. The pap smear has virtually eliminated cervical cancer but dealing with an abnormal PAP is stressful and costly. Cervical bleeding problems also make for an unhappy patient. During the LIH procedure a donut hole like incision is made to remove the cervical canal. The cervical tissue is closed with suture. LIH reduces the risk of cervical cancer along with bleeding while still leaving the pelvic floor anatomy, nerve supply and blood flow as close to normal as possible.
FAQs on Hysterectomy Alternatives
I’m unsure about getting a hysterectomy. Do I have any alternatives?
All women’s medical societies recognize a woman’s right to choose, and no woman should be told hysterectomy is her only option for a benign problem. For example, regardless of age a woman with fibroids can have myomectomy. Prolapse repairs do not require hysterectomy. For bleeding problems, endometrial ablation is a well-established alternative to hysterectomy.
What are the alternatives to a hysterectomy procedure?
Depending on your condition, preferences, and goals, there may be a number of alternative options to which you can turn for relief. Below is a list of the alternative GYN procedures we offer at Advanced Women’s Health Institute:
- Hysteroscopic Myomectomy/Polypectomy: When abnormal bleeding is caused by fibroids or polyps growing into the uterine cavity they can be removed with minimal discomfort. Women are back to work in 2-3 days and all normal activities in one week on average. Hysteroscopic surgery will correct the bleeding problem with less pain and risk than hysterectomy. This is especially important for the woman who wants to maintain fertility.

- Endometrial Ablation: Endometrial ablation is an alternative to hysterectomy for abnormal uterine bleeding.
- Endometrial Resection Ablation (ERA): The same scope used for hysteroscopic myomectomy and polypectomy is used to remove the uterine lining, thus eliminating menstrual flow. Return to work is also 2-3 days and complete recovery is one week on average. The average woman waits 4 weeks to return to work after a vaginal hysterectomy. Three randomized controlled trials comparing ERA to vaginal hysterectomy concluded, overall, patients were equally satisfied with their surgery after one year or more. ERA is considered the gold standard of endometrial ablation. Women who have multiple fibroids or other pathology may want to consider other minimally invasive approaches.

- Global Ablation: In the last several years devices have been developed to make endometrial ablation easier to perform so general OB/GYN’s can offer this less invasive, less painful treatment for abnormal bleeding to their patients. These devices use various forms of energy to destroy the uterine lining, including:
- Balloon Therapy
- Hot saline infusion
- Cryoablation
- Microwave Ablation
- Electrocautery
Global ablation is a less invasive, less painful alternative to hysterectomy, but is not considered the”gold standard” of ablation.. ERA is a sub-specialty procedure. It is the most effective alternative to hysterectomy to stop bleeding, and ERA can be relied on for permanent sterilization.. For a state-of-the-art ablation procedure, schedule your appointment with the Advanced Women’s Health Institute.
Do I always need a hysterectomy to remove fibroids?
Fibroids that are too large for hysteroscopic myomectomy can be removed without the need for hysterectomy. Surgical alternatives to hysterectomy for fibroids include:
- Open abdominal myomectomy: Through a 4-8 inch abdominal incision, fibroids are removed and the uterus is closed with suture. Women can successfully get pregnant after myomectomy. The procedure has been described in the medical literature for over 100 years. Myomectomy is safe when performed by an appropriately trained physician. Return to work is usually 6 weeks, though complete recovery can take longer.
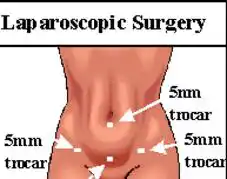
- Laparoscopic myomectomy: A pencil-sized (5mm) scope placed through the base of your belly button sends a video image to the monitoring screen while the myomectomy is completed using small, minimally-invasive instruments. This form of myomectomy is outpatient instead of 2-4 days in hospital. We have reported return to work is possible in 10 days for our average patient, not 6 weeks as in a fully-open surgery. The average woman who has laparoscopic myomectomy states she feels fully recovered in 3 weeks.

- Laparoscopic myomectomy with endometrial ablation: For the woman who would prefer not to undergo a hysterectomy, but would like to terminate menstrual flow, the uterine lining can be removed at the same time as laparoscopic myomectomy.
- Uterine artery embolization (UAE): First described in the mid 1990’s, a catheter is inserted into the femoral artery at the top of your leg and guided to the uterine arteries with a live x-ray. Polyvinyl chloride particles will be infused until blood flow no longer can be detected, causing any fibroids to shrink. The majority of women report significant pain, like childbirth for 12-24 hours afterward. One study concluded women who had laparoscopic myomectomy were more satisfied with their outcome than those with UAE.
- MRI-guided high intensity focused ultrasound: Although approved by the FDA, this procedure cannot treat more than 1-2 fibroids at a time in a 2-3 hour procedure. This is costly and typically is not covered by insurance. The patient with the larger uterus and multiple fibroids would require 2 or more procedures.
- Uterine artery occlusion: This is described as a laparoscopic procedure to accomplish the same end result as UAE.
- Myolysis: This was described around 1990 as a laparoscopic procedure to shrink fibroids. It was the first laparoscopic alternative to hysterectomy. To shrink the fibroid, either a laser fiber or a bipolar cautery needle was inserted many times into different locations throughout the tumor. The fibroid gets smaller over the next several weeks. It became less attractive to patients once laparoscopic myomectomy became possible..
- Laparoscopic radio frequency ablation: This is a new laparoscopic procedure to accomplish the same end result as myolysis, It appears more effective than myolysis because only one insertion is made. More studies are needed to understand its benefit. It may be difficult to get covered by insurance since it is new. It is an alternative to hysterectomy if laparoscopic myomectomy is not an available option.
- SONATA: SONATA is a non-laparoscopy radio frequency ablation procedure. No incisions are required.. An ultrasound probe is placed inside the uterus to visualize the fibroids. Under ultrasound guidance a needle is inserted into a fibroid. The ablation is performed and the fibroid shrinks in size over several weeks. It is difficult to treat larger fibroids with SONATA. Also, fibroids that protrude out of the uterus cannot be treated. In some cases SONATA would be combined with laparoscopic and/or hysteroscopic myomectomy. More studies are needed to understand its benefit. It may be difficult to get covered by insurance since it is new.
A complete and thorough evaluation is important to the success of any surgery, and every patient is an individual. Dr. Moore and the team will work closely with you to determine your needs and goals in order to help you choose the right procedure.